Treatment induced lymphedema in oral cancer patients: A wolf in sheep’s clothing.
Purpose/Objective
1. To study the incidence and the course of development and regression of head and neck lymphedema(HNL) in patients undergoing curative treatment for oral cancer.
2.To study the effect of HNL on airway, speech and swallowing functions immediately and after 6 months of treatment
Material/Methods
A prospective observational study was conducted in the Department of Head and Neck Oncology, and the Department of Radiotherapy in Dr. B.Borooah Cancer Institute, Guwahati, over a period of 1 year. Ethical committee approval was obtained prior to commencing the study. All patients undergoing treatment for oral cancer with the curative intent, by means of Surgery +/- Adjuvant therapy, with or without Neoadjuvant Chemotherapy were included in the study. Any recurrent cases, or patients developing recurrent or residual disease were excluded from the study. Patients with pre op overt hypothyroidism, chronic kidney disease, chronic liver disease, severe burns or scars in head and neck region were excluded from the study; as these would affect lymphedema scores. Also, patients with pre operative dysphonia or dysphagia due to any cause other than oral cancer were excluded from the study to avoid any bias in dysphonia/dysphagia scores during follow up.
Details of staging, pre-treatment disease volume, surgery and its extent, adjuvant therapy, radiation fields, techniques and dose, chemotherapy dose and schedule were recorded. MD Anderson Head and Neck Lymphedema Rating Scale for external lymphedema and Modified Patterson scale for internal HNL were used to analyze the lymphedema scores.1-2 External lymphedema was evaluated clinically, whereas internal lymphedema was evaluated by analyzing the videographic recordings of flexible laryngoscopy. Voice Handicap Index and MD Anderson Dysphagia Inventory for dysphagia evaluation, were used to evaluate dysphonia and dysphagia.3-4 Evaluation of these parameters were done at each follow up visit, as per the institution’s follow up protocol. Range of motion in neck and mobility oral/pharyngeal structures were evaluated at each follow up. Repeat imaging was done was as per institutional protocol/ as and when indicated.
Patients were classified into 2 groups:
- Patients undergoing surgery, with no adjuvant therapy
- Patients undergoing surgery, with adjuvant therapy(RT+/-CT)
The effect of NACT on HNL was evaluated separately.
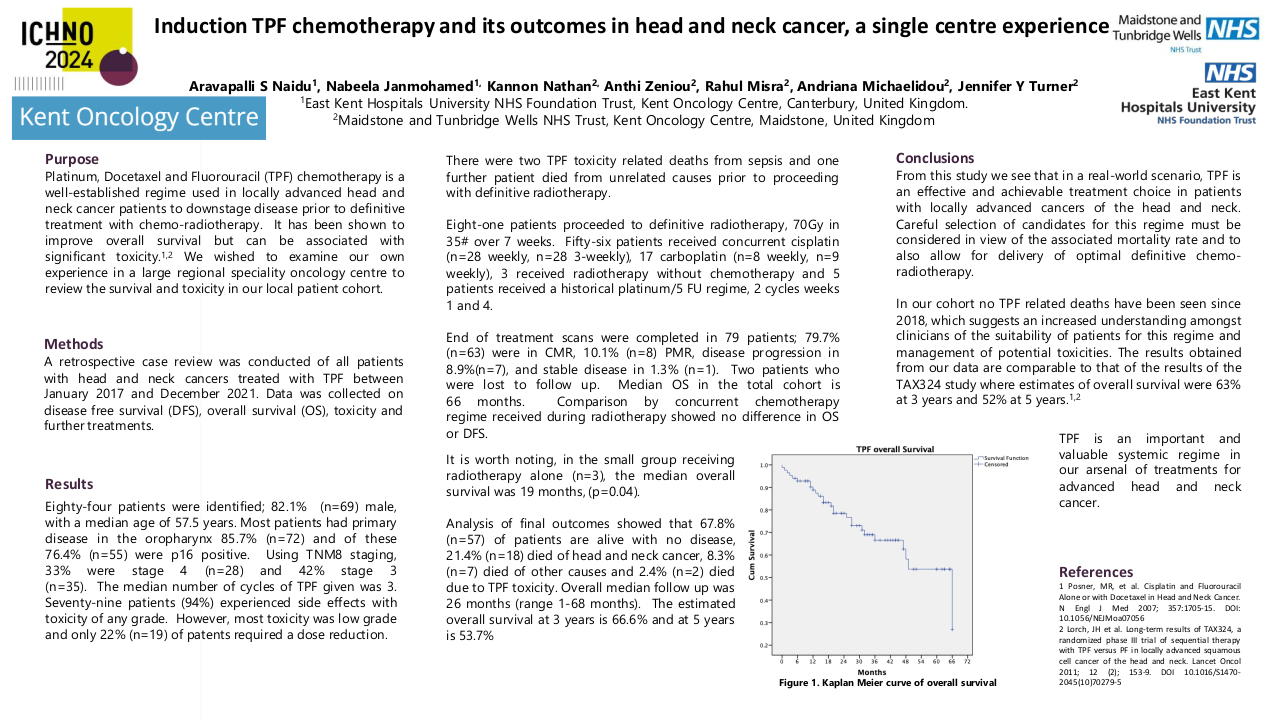
Results
A total of 98 patients were included in the study, of which 17 patients were excluded from the analysis due to residual/recurrent disease/ death/ lost to follow up.
Out of 81 patients, 28 underwent surgery alone, with no adjuvant therapy. At the initial presentation, 76% patients had combined external and internal lymphedema. The extent of lymphedema was determined by the pattern of growth (infiltrative vs proliferative), and extent of resection. Extent of glossectomy (type I vs Type II or beyond, p=0.037), segmental mandibular resection(p=0.039) significantly affected internal lymphedema scores. Extent of neck dissection, choice of reconstruction, maxillectomy and tumor volume did not affect lymphedema scores at the end of 6 months. External edema in most patients subsided by the end of 2nd follow up, at around 3 months after surgery. Internal edema, however persisted in 59% of the patients at the end of 3 months, and 14% patients at the end of 6 months. Highest internal lymphedema scores were recorded for base of tongue in the initial (3.21) follow up and at the end of 6 months (0.94). Dysphagia and dysphonia scores correlated with internal lymphedema scores.
Out of 81 patients, 53 patients were included in the surgery with adjuvant therapy group. A total of 44 patients received radiation alone, and 9 patients received chemoradiation. 86% patients had combined external and internal lymphedema at first presentation. Addition of chemotherapy did not show any statistically significant difference in the lymphedema scores. The field of radiation, pathological nodal status (pN0 vs pN+, p=0.034) and extent of glossectomy statistically affected the lymphedema scores at the end of 6 months. External lymphedema scores dropped by the end of 4-6 months in 84% patients, whereas internal lymphedema persisted in 63% patients. There was no statistically significant difference between base of tongue and other subsites of laryngopharynx with regard to internal lymphedema. The dysphagia and dysphonia scores were worse in this group, however, they correlated with internal lymphedema scores. The proportion of patients requiring manual lymphatic decompression therapy was higher in surgery with adjuvant therapy group vs surgery only group ( p= 0.00026).
Conclusion
HNL is a commonly encountered, yet often neglected effect of curative treatment in early and locally advanced oral cavity. The behaviour of HNL in early and advanced oral cavity cancers following treatment may differ. Internal lymphedema may contribute to dysphagia and dysphonia in these patients.
1. Smith BG, Hutcheson KA, Little LG, Skoracki RJ, Rosenthal DI, Lai SY, Lewin JS. Lymphedema outcomes in patients with head and neck cancer. Otolaryngol Head Neck Surg. 2015 Feb;152(2):284-291. doi: 10.1177/0194599814558402. 2. Starmer HM, Drinnan M, Bhabra M, Watson LJ, Patterson J. Development and reliability of the revised Patterson Edema Scale. Clin Otolaryngol. 2021 Jul;46(4):752-757. doi: 10.1111/coa.13727. 3. Barbara H. Jacobson, Alex Johnson, Cynthia Grywalski, Alice Silbergleit, Gary Jaconsen, Michael S. Benninger. The Voice Handicap Index (VHI): Development and Validation. American Journal of Speech-Language Pathology, Vol 6(3), 66-70, 19974. Chen AY, Frankowski R, Bishop-Leone J, et al. The Development and Validation of a Dysphagia-Specific Quality-of-Life Questionnaire for Patients With Head and Neck Cancer: The M. D. Anderson Dysphagia Inventory. Arch Otolaryngol Head Neck Surg. 2001;127(7):870-876.