Selected inoperable oral cavity cancers may be salvaged using definitive radiotherapy (RT) and chemo-radiotherapy (CRT): A single center experience.
Purpose/Objective
Upfront surgical resection is considered as standard curative treatment in oral cancers with radiotherapy (RT) being used as adjuvant in locally advanced cases. The prognosis of surgically unresectable patients is considered poor and palliative options are offered. Institutional series on treatment of oral cancers with definitive radiation therapy or chemo-radiation (CRT) often include a mix of surgically unresectable and medically inoperable patients. The primary objective of this study was to report the outcomes of definitive non surgical therapy in locally advanced unresectable oral cavity squamous cell carcinoma (LA-OCC).
Material/Methods
We retrospectively examined patients with Stage III/IV previously untreated, non-metastatic, surgically unresectable LA-OCC treated definitively from 2011 to 2021.Following multidisciplinary discussions such patients were offered RT or CRT with or without neoadjuvant chemotherapy (NACT). NACT was offered only when the multidisciplinary team (MDT) felt that the disease burden was heavy and the patient's performance score (PS) was optimal, to tolerate definitive RT post NACT. A dose of 66Gy/30Fr/6 weeks with concurrent weekly cisplatin 40mg/m2 or 55Gy/20Fr/4 weeks with RT alone was prescribed. Overall and progression free survival (OS, PFS) and treatment toxicities were analyzed.
Results
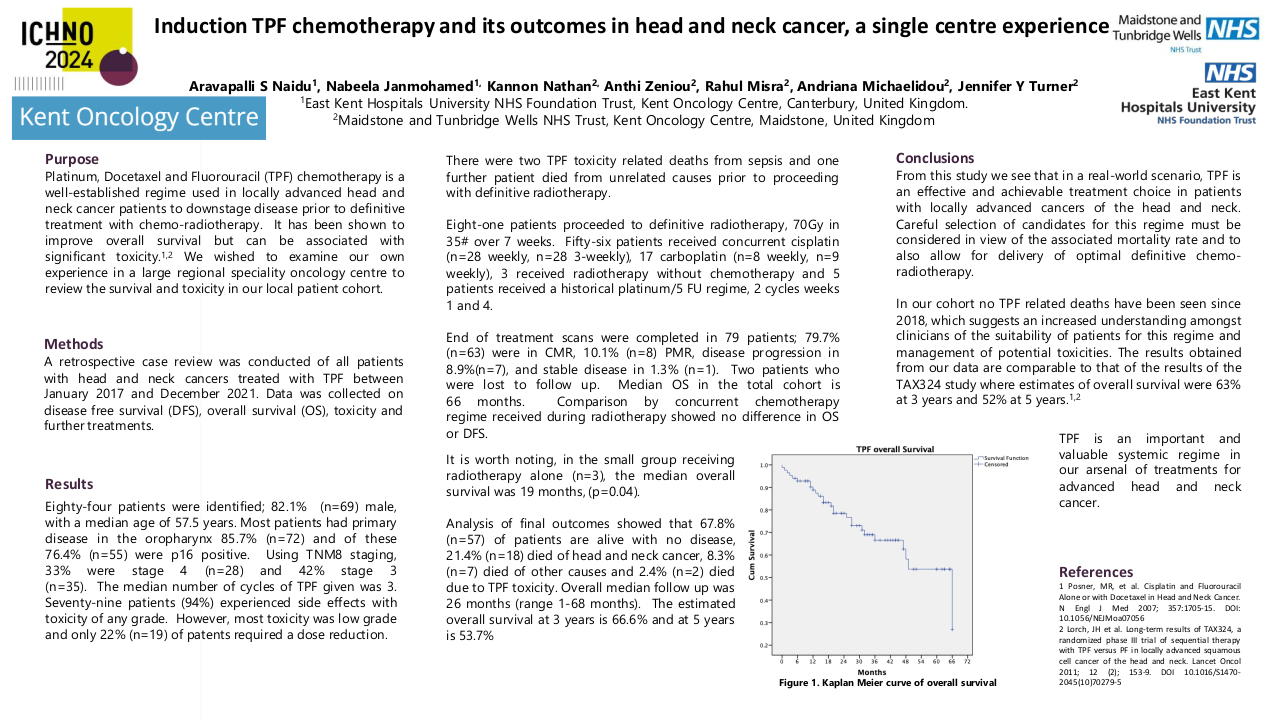
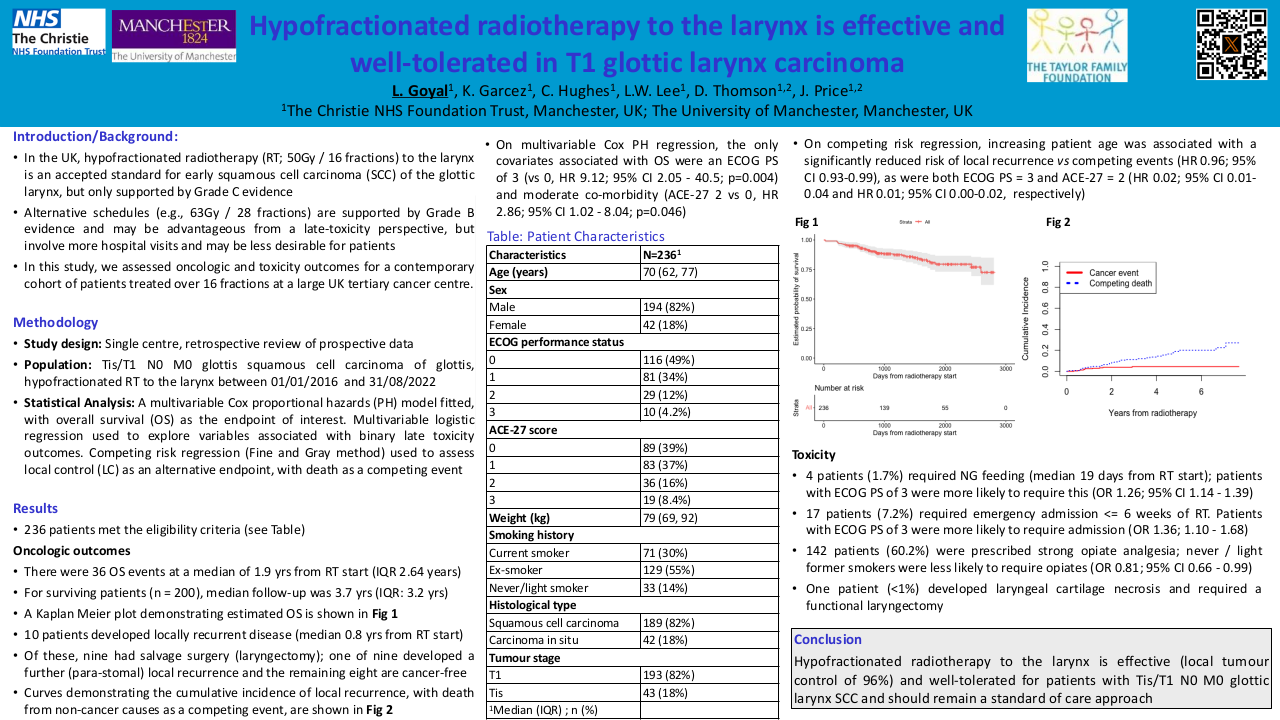
Sixty-nine patients met the inclusion criteria, median age 54 years (range 27-86) of whom 59 (85%) were males. Oral tongue was the most common (38%), followed by buccal mucosa (32%), hard palate (13%), and others (17.3%). T4a, T4b, N2-3 disease was present in 28 (40.6%), 26 (37.7%) and 39 (56.5%) patients respectively. The commonest causes for unresectability were high ITF/ base of skull involvement (47.8%) and extension into oropharynx (42%). There were four distinct treatment cohorts: Cohort A: NACT + CRT (n = 26, 37.6%); B: NACT + RT (when not fit for CRT post NACT; N = 6,8.6%), C: CRT (N=15,21%) and D: only RT (N=22, 31.8%). The median follow up was 10 months. Median OS and PFS of the whole group was 16 months with a 95% CI (8.8 -23.2 months) and 10 months 95% CI (7.7-12.3 months). The projected loco-regional control at 1 year, 2 years and 3 years were 63.8%, 60.4% and 45.3% respectively The median OS of cohort A was 16 months (7.5-24.4), cohort B was 8 months (3.5-12.5) , cohort C was Not Reached and cohort D was 21 months respectively. There were no differences in outcomes based on bone involvement or NACT. Seventeen patients (25%) needed admissions for toxicities and nasogastric tube insertion was required in 32 patients (47%). There were nine (13%) early deaths within three months of completion of RT/CRT, majority (66.5%) attributable to disease progression.
Conclusion
Carefully selected patients LA-OCC cancers respond well to definitive intent RT/CRT with acceptable toxicities. NACT may be used in selected patients, however in patients who remain unfit for CRT post NACT, outcomes are poor.