Re-irradiation in head and neck cancers: Real-world experience from a tertiary cancer institute
Purpose/Objective
More than 1/3rd of head and neck cancer patients eventually fail loco-regionally or appear as second primary, despite ever-improving treatment options.1,2 Recommended potentially curative treatment options include salvage surgery if the disease is amenable to surgery, or reirradiation.2 Reirradiation of head and neck cancers presents a dilemma in terms of achieving adequate doses to the target, maintaining the organ-at-risks (OAR) dose constraints within limits, and managing toxicities emerging during and after the treatment.3–5 Intensity-modulated radiotherapy (IMRT) has slowly evolved to be the modality of choice for re-irradiation owing to its ability to improve disease control and reduce treatment-related toxicity.6 We present the data of re-irradiated head and neck cancer patients treated at our centre with IMRT.
Material/Methods
This was a retrospective single-arm observational analysis. Details of head and neck cancer patients treated at our hospital with re-irradiation were retrieved. After reviewing all the treatment records, the follow-up details were assembled.
All the cases were treated with IMRT with or without concurrent chemotherapy. All the patients received radiation and re-irradiation with a dose-per-fraction of 1.8 to 2Gray with adjuvant or definitive intent, for five days a week for six weeks or above. The dose prescribed was preferably 60 – 66Gy in 30-33 fractions. Dose constraints used for OARs were: Spinal cord Dmax <=45Gy, and brainstem and optic apparatus Dmax <=54Gy.3,5 Special care was also taken to limit the cumulative dose of carotid arteries to <120Gy.7 The mean dose of parotid was limited at 23Gy, although target volume coverage was given priority, whenever the two were in proximity.
Patients were immobilised using a 5-clamp head and neck thermoplastic mask. 3 mm slice thickness contrast-enhanced computed tomography (CT) images were obtained from vertex to 2 cm below the carina using Siemens Emotion 6 (Somatom, Germany). The treatment planning was done on MONACO (Version 5.11). The target volumes for definitive treatment were contoured as per ICRU 62.8 The decision to include nodes depended on certain factors: previous history of nodal positivity, nature of irradiation in the first radiotherapy schedule, nature and location of primary during second irradiation, definitive/adjuvant intent of re-irradiation, surgical resection of nodes, duration between the irradiation treatments, dose volumes used and dosimetric parameters achieved for OARs in the first radiotherapy.
Patients were treated by using linear accelerator (Elekta Compact and Synergy; Elekta, Crawley, UK). All patients were followed up on a regular basis. Response assessment scans were done after 3 months of treatment completion.
Overall Survival (OS) was defined time from start date of re-irradiation to the date of death or date of last clinical follow-up. Progression-free survival (PFS) was defined as interval from the start date of RT to any documented recurrence. Analysis was performed with the SPSS statistical (version 23.0; IBM, Armonk, NY, USA). All potential prognostic factors were analysed. the patients were divided into three prognostic subgroups using Multi-Institution Re-irradiation (MIRI) recursive partitioning analysis (RPA).9
Results
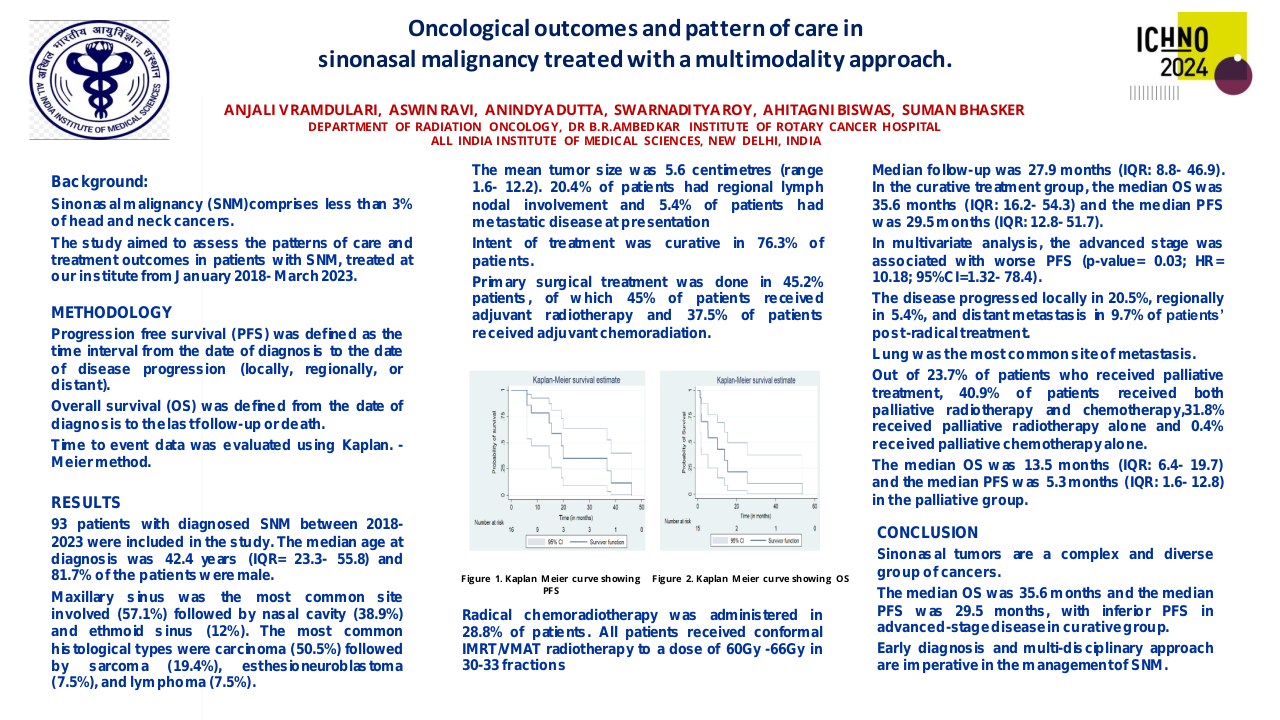
Seventy-three cases were included in the final analysis. During the re-irradiation schedule, 34/73 cases were treated with definitive irradiation, whereas 39 cases were treated with postoperative adjuvant radiotherapy. Median interval between both the RT schedules was 55 months (range: 13-197). Median follow-up duration after re-irradiation was 23 months (range: 4-74). Median initial RT dose was 60 Gy (range: 58-66) and median re-irradiation dose was 60Gy (range: 54-66). The median initial RT and re-irradiation dose was 2Gy (range: 1.8-2).
There were 41 events in PFS. The 2-year and 4-year PFS rates were 55.8% and 29.2%. The estimated 4-year DFS definitive re-irradiation versus adjuvant radiotherapy were 28.7 vs 29.3% (p-0.786).
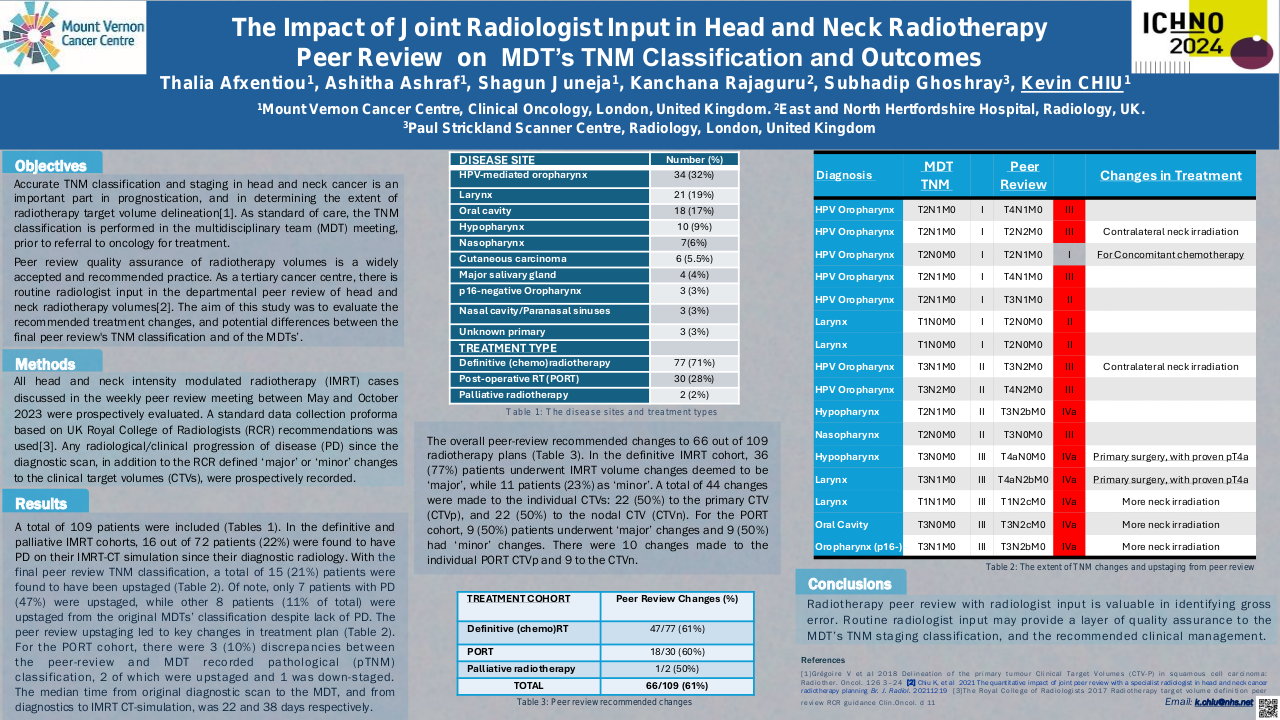
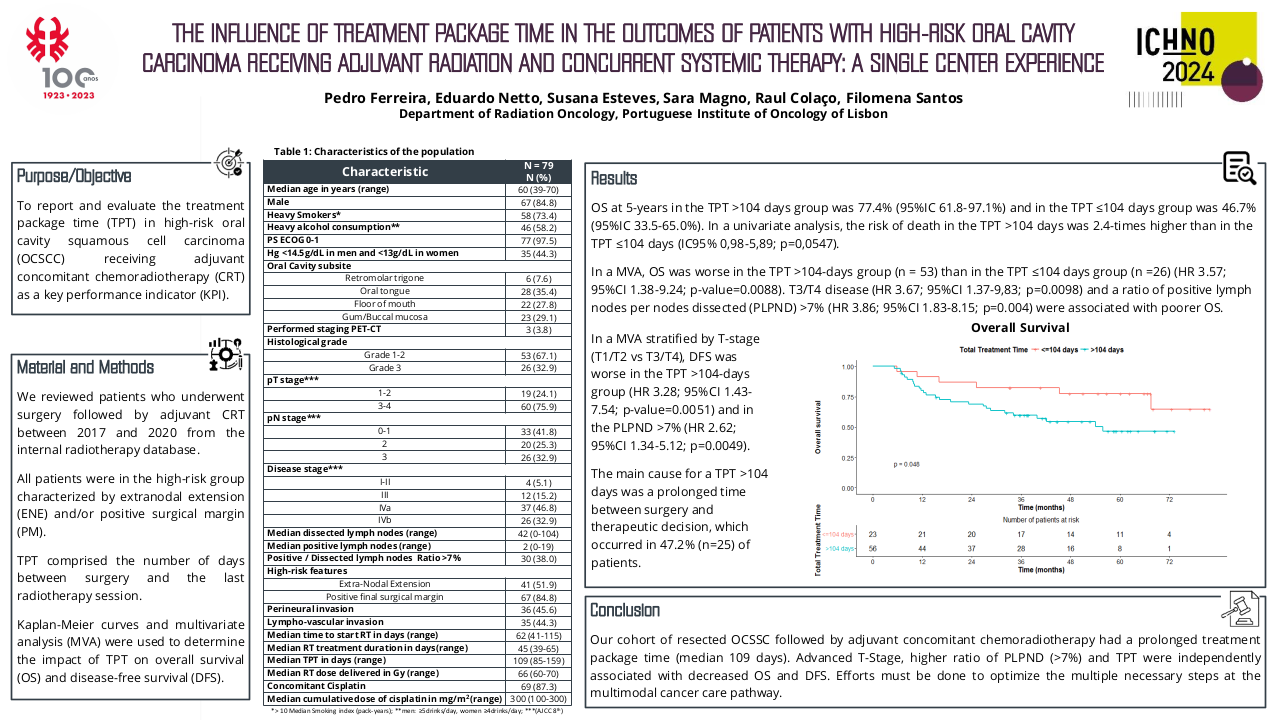
There was no statistically significant difference for 3-year OS of de novo versus post-operative cases (54.7 vs 56.3%, p-0.559). No significant differences in DFS or OS were elucidated for duration of re-irradiation for a 2-year period (48.6 vs 39.7, p-0.648) and 3-year period (3yr DFS – 48 vs 57.5%, p-0.091).
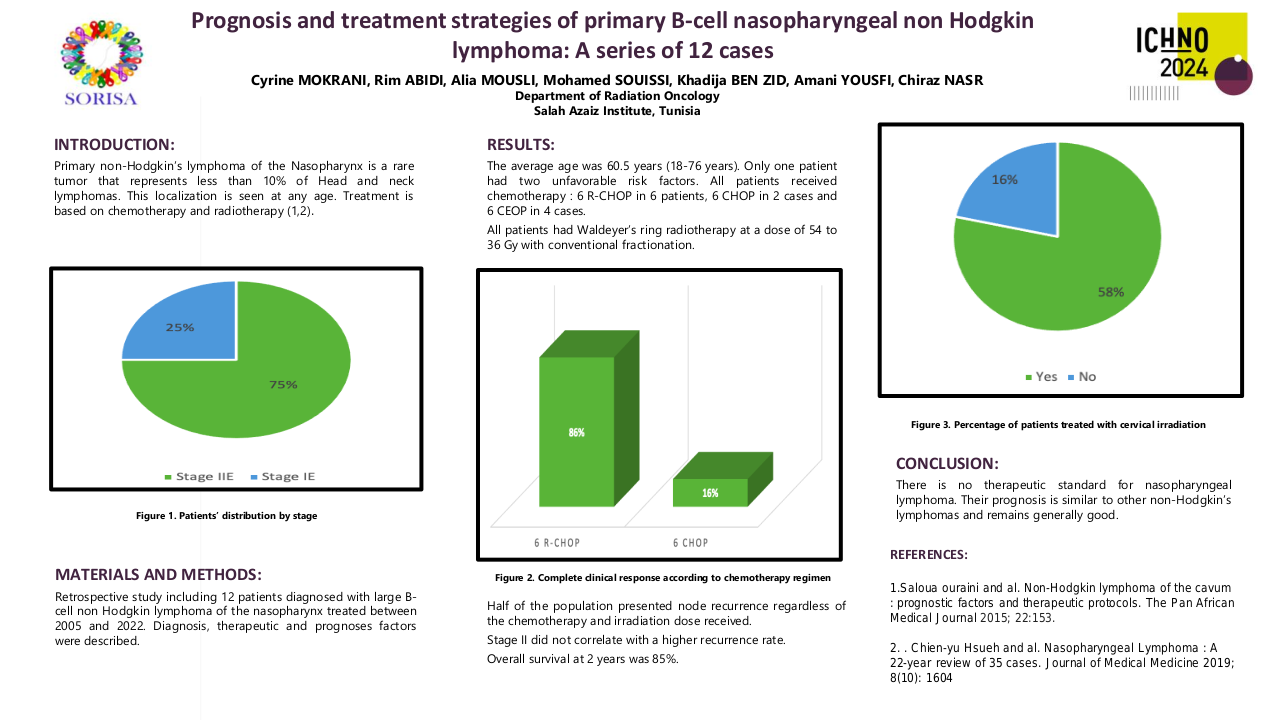
Patients recurring within 2 years of primary radiation had poorer OS than those recurring after 2 years. (57.14 vs 49.25%, p-0.039). Patients with more than 3 high-risk factors during adjuvant reirradiation post-surgery had poor OS. (38.46 vs 31.5%, p-0.043). The number of cases in RPA Class I, II, and III were 16, 49 and 8, respectively. The 2-year DFS for Class I, II and III, were 62.5%, 59.7% and 12.5% (p<0.0001).
Conclusion
Re-irradiation in head and neck cancers is tolerable and toxicities are acceptable. A larger cohort and a longer duration of study will help in discerning the factors that will help in reducing the toxicities and improving outcomes further.
1. Bots WTC, van den Bosch S, Zwijnenburg EM, et al. Reirradiation of head and neck cancer: Long-term disease control and toxicity. Head Neck. 2017;39(6):1122-1130. doi:10.1002/hed.247332. Kim YS. Reirradiation of head and neck cancer in the era of intensity-modulated radiotherapy: patient selection, practical aspects, and current evidence. Radiat Oncol J. 2017;35(1):1-15. doi:10.3857/roj.2017.001223. Benson R, Giridhar P, Venkatesulu BP, Mallick S, Raza MW, Rath GK. Re-irradiation for head and neck squamous cell carcinoma. J Egypt Natl Canc Inst. 2017;29(1):1-9. doi:10.1016/j.jnci.2016.07.0024. Popovtzer A, Gluck I, Chepeha DB, et al. The pattern of failure after reirradiation of recurrent squamous cell head and neck cancer: implications for defining the targets. Int J Radiat Oncol Biol Phys. 2009;74(5):1342-1347. doi:10.1016/j.ijrobp.2008.10.0425. Lee N, Chan K, Bekelman JE, et al. Salvage re-irradiation for recurrent head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;68(3):731-740. doi:10.1016/j.ijrobp.2006.12.0556. Re-irradiation Using Intensity-modulated Radiotherapy for Recurrent and Second Primary Head and Neck Cancer. Anticancer Res. 2018;38(5). doi:10.21873/anticanres.125807. Embring A, Onjukka E, Mercke C, et al. Re-Irradiation for Head and Neck Cancer: Cumulative Dose to Organs at Risk and Late Side Effects. Cancers (Basel). 2021;13(13). doi:10.3390/cancers131331738. Stroom JC, Heijmen BJM. Geometrical uncertainties, radiotherapy planning margins, and the ICRU-62 report. Radiotherapy and Oncology. 2002;64(1):75-83. doi:10.1016/S0167-8140(02)00140-89. Ward MC, Riaz N, Caudell JJ, et al. Refining Patient Selection for Reirradiation of Head and Neck Squamous Carcinoma in the IMRT Era: A Multi-institution Cohort Study by the MIRI Collaborative. Int J Radiat Oncol Biol Phys. 2018;100(3):586-594. doi:10.1016/j.ijrobp.2017.06.012